Quo Vadis, Philippine Health: Why our health system continues to fail to serve the poorest

Doctor Alberto “Quasi” del Gallego Romualdez took over the Department of Health (DoH) in 1998 as President Erap Estrada’s Health Secretary. He told DoH employees in his first meeting “When he appointed me, President Estrada’s instruction was simple: Make sure that the DoH serves the people, especially the poor… I know that all of you understand this to be the department’s true mission in the first place.” Having been in and out of DoH since 1988 and acting as adviser to previous Health Secretaries Flavier, Galvez Tan, Reodica, and Estrella since 1992, he decided to take on the job himself. And he had a dream to reform the health sector to serve the poorest Filipinos.
Just a few years before he took over the DoH (1991), the National Statistical Coordination Board had approved a system to measure how much the country was spending on health and who was paying. When the first (1995) National Health Accounts came out, it was an eye opener for the DoH. (See Table 1.)

Government could do nothing about reducing healthcare costs for the poorest, as even the Secretary of Health only had a 20% share in the health expenditure of the country, with half its budget transferred to local governments.
Secretary Quasi wanted to reverse spending in the health sector to remove the burden of health (which he considered a human right) from individuals, particularly the poorest. He called it Health Sector Reform (others would add Agenda later); it has therefore been referred to as the HSRA.
It was a simple equation: to relieve the poor of financing their health needs, he would increase government spending for health, increase Medicare (PhilHealth) reimbursements for hospital and outpatient care, starting with the most vulnerable poor who had the largest burden of disease. He would flip health financing and reduce household payment to a minimum of 20%. (See Table 2.)
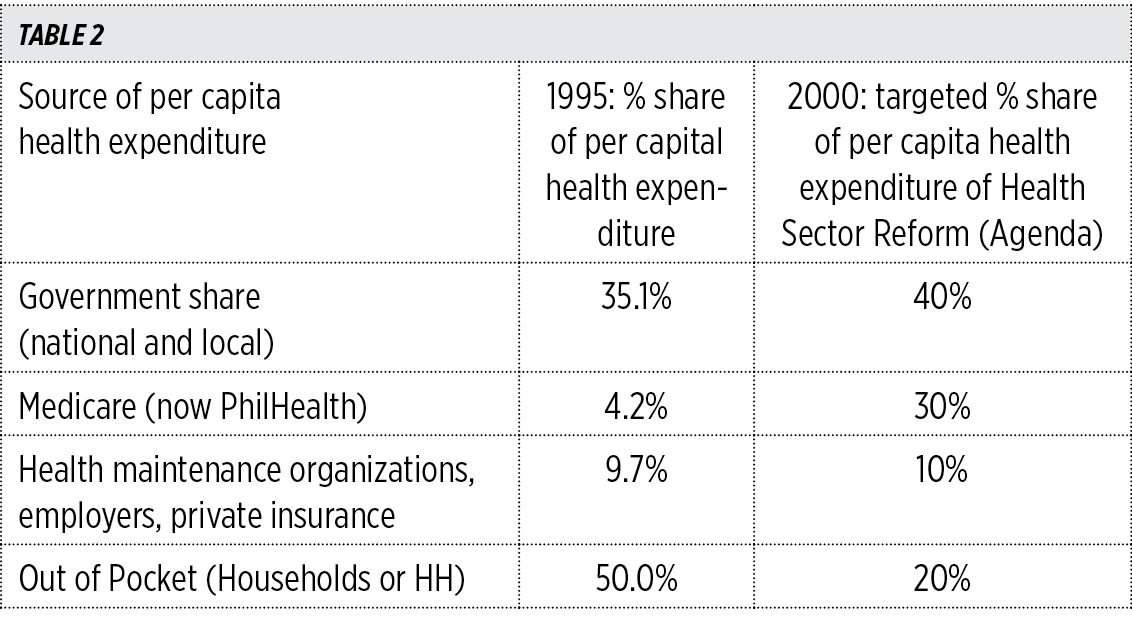
Secretary Quasi also believed that PhilHealth should cover everyone’s health needs (universal health insurance) and that this should be based on primary healthcare. Local governments would develop a decentralized healthcare system, from the bottom up to achieve health for all.
In March 1999 he called for a health summit of provincial governors and agreed to a partnership with local government units (LGUs), the Department of the Interior and Local Government (DILG), and the DoH. The resulting Health Covenant 1999 would create a National Health Planning Committee to achieve an integrated healthcare system by 2000, facilitating National Government transfers to LGUs through co-funding of more efficient and effective area plans of governors and city mayors. President Estrada approved the National Health Planning Committee through Executive Order 205 on Jan. 31, 2000.
The next agenda would be to rapidly increase health financing through Universal Health Insurance to achieve HSRA. Without yet benefit of a law to improve health financing, but with the LGUs behind him, he succeeded in increasing LGU financing and reducing Out of Pocket (OOP) spending by 2000. (See Table 3.)

Secretary Quasi was able to show during his term that increased government spending and social health insurance would lead to reduced out of pocket spending, bringing down health costs for all.
But after two decades of health sector reform and with sin taxes and a Universal Health Care (UHC) law in place, succeeding administrations have failed to even maintain Sec. Quasi’s modest successes. (See Table 4.)
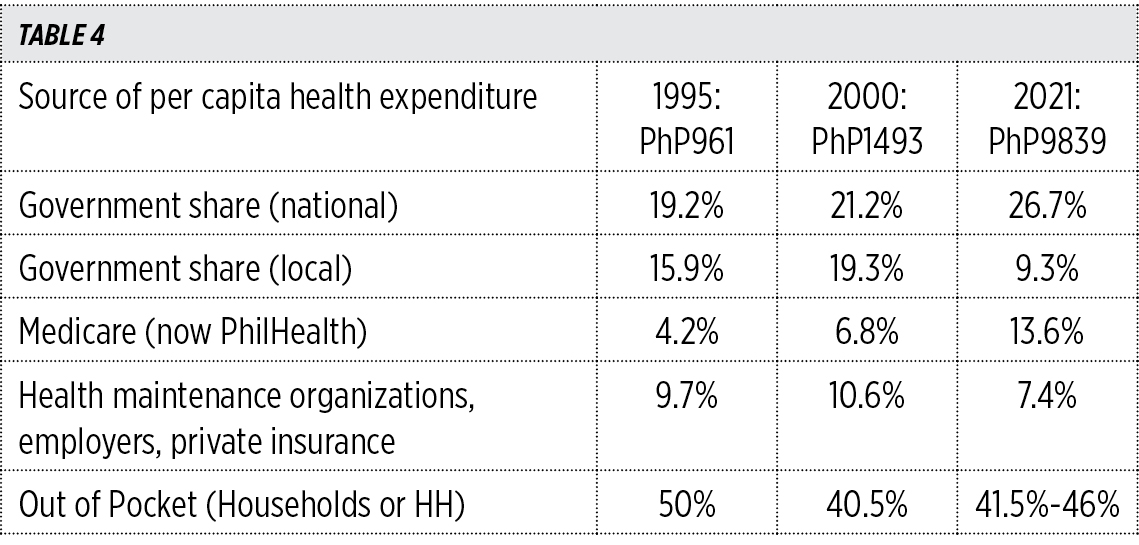
We are now spending 6.6 times more for health after 20 years and still individually pay for P45 out of every P100 of health care. Not much different from 2000.
LOCAL GOVERNMENTS AND THE NATIONAL HEALTH SECTOR: FROM PARTNERSHIP TO COMPETITION
Far from the partnership agreement in 2000 between the DoH and LGUs for an integrated health system, the DoH now struggles for a formula to make universal healthcare work for local health systems run by LGUs which see National Government programs as more unfunded impositions and its facilities as competitors for PhilHealth reimbursements.
Despite the presence of a local health system run by LGUs that the rural and urban poor could depend on, local governments have underinvested in local clinics and hospitals as the National Government spent P277 billion on health in 2021, almost three times what local governments spent on health, at P97 billion (2021 PNHA, PSA).
When the health sector reform was at its height in 2003, LGUs were spending 20% of their Internal Revenue Allotment (IRA) on health (P23.5 billion out of P113 billion). By 2021 this had declined to 13.9% of IRA (P97 billion out of P695 billion). By 2022 the health sector was competing with 19 other sectors for local funding (there were only four sectors at the time of devolution in 1993).
From a 20% LGU share of Current Health Expenditure in 2000, LGUs now cover only 9.3% of health spending (2021 PNHA, PSA). This resulted from a deliberate national policy under the Arroyo administration to leave local governments on their own from 2001-2010. As a first declaration of this policy, without Secretary Quasi at the helm of the DoH, President Gloria Macapagal-Arroyo rescinded Executive Order 205, ending the budding partnership with LGUs.
The Arroyo administration would be the subject of debate by the 2004 presidential elections when it was shown that health budgets were declining and even unused, particularly for family planning, as Congress continued to debate the Reproductive Health Law.
In a May 2013 presentation titled “Decentralized Spending and Intergovernmental Transfers in the Philippines,” Rosario Manasan noted that it was “worrisome that real per capita LGU expenditures (for all LGUs in aggregate) on social services and economic services declined/stagnated from a peak in 2000.”
Instead of financing local health systems, the focus of PhilHealth under President Arroyo would be on expanding membership, with the national health insurance program asking LGUs to pay for the membership of its poor constituents. Some governors were quick to point out that most PhilHealth payments were going to better equipped and fully staffed DoH national hospitals, leaving little for ill equipped and staffed LGU hospitals.
During this decade of (unhealthy) health competition, the distribution of PhilHealth cards became a staple in political rallies, with faces and names of politicians covering much of the membership cards, which people would soon find out would be good only for a year and would carry no benefit in hospitals and clinics without medicines, supplies, and qualified staff.
The administration of President Noynoy Aquino would have to deal with the previous administration’s neglect of the health system by hiring doctors, nurses, and midwives for understaffed and underfunded local health facilities. The expansion of the Health Facility Enhancement Program under his administration to a national program would become a battleground for competing political interests, with local governments usually losing out to Congressional representatives and senators for a share of much-needed health infrastructure. The Responsible Parenthood Reproductive Health law would only see minimal funding as the Senate continued to resist its full implementation, and Philippine Commission on Population, the DoH and the LGUs would have the same limited resources year after year.
The great promise for the future funding of the health system would now have to be with the Sin Tax Law. The DoF projects that from P143 billion collected in 2015, current versions could be expected to reach P600 billion by 2024 (from the Department of Finance website).
Under the Duterte administration, LGUs would continue to compete on health service delivery with DoH hospital-based Malasakit and similar programs. This forced the poor to travel to hospitals as community-based health programs continued to survive with the same funding while the population’s number, including the poorest, increased in number. Local governments still have the same number of health workers today when our population has increased to 110 million, as it had at the start of devolution in 1993 when the population was 65 million.
The 2019 UHC law seeks to integrate local health services under provincial governors and city mayors, a reprise of what Secretary Quasi started in 2000. The UHC law also has to set up this integrated system, this time based on PhilHealth reimbursements and the Sin Tax revenues rather than investments by local governments. As this is still an evolving system, local investments in health (P97 billion) may be in jeopardy if the DoH would take too long crafting “sandbox” projects in half a dozen LGUs.
It is most stark when 22% (11.4% female) of Filipinos seeking healthcare are 60 years and older (they only make up 10% of the population) and 59% of the expense for their treatment comes out of their pockets. Further, 14% of health expenditures in 2018 went to those 65 years and older, the largest expense for any age group (2018 PNHA, Health expenditures of the most vulnerable population segments).
The poorest Filipinos belonging to the lowest incomes have been increasing their share (out of pocket or OOP) for their healthcare in the last seven years. The OOP share of the poorest quintile has increased by 2.1% (a larger increase than the second and third quintiles taken separately) while the richest quintile has seen a decline in its share of the OOP by 5.3% from 2014-2020. The two poorest quintiles now have a 31.1% share of OOP, from 27.5% in 2014.
The US Agency for International Development (USAID) Health Protect notes:
“Assuming that other national agencies will reduce spending on health and COVID-19 response in 2022, the percentage spending (for health) could decline to 16.6% in 2022 and 17.3% in 2023 based on DoH budget levels. This would imply that the decline in OOP is unlikely to continue from 2022 onwards and can go back to its pre-pandemic levels at 48.7% in 2022 and 47.9% in 2023.”
Government cannot be lulled by the current decline in the pandemic, which served to expose the weakness of the current health system.
Secretary Quasi, who died in 2013, would be livid at the current health situation of the country. As all Filipinos should be.
Jeepy Perez specializes in public health administration and primary healthcare. He was undersecretary for Population and Development and executive director of the country’s Commission on Population and Development up to Sept. 8, 2022. He occasionally writes for Action for Economic Reforms.


